Exploring Networks of Health
Posted on April 12, 2011 | posted by: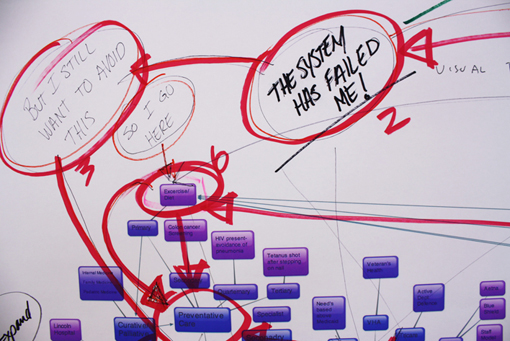
by Francis Carter, Minuette Le & Jayson Rupert
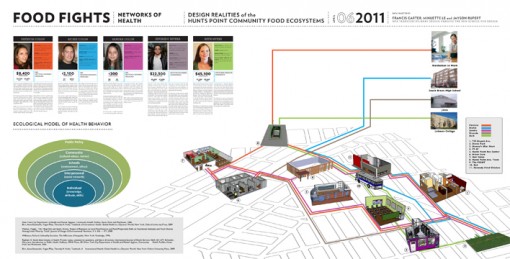
Reimagining the Hunts Point food systems requires a closer look at the Networks of Health and the totality of how this system serves and functions within the community. The rates of obesity, diabetes, and asthma for residents living in Hunts Point are alarmingly high. Additional health concerns specific to the Hunts Point Community are the statistics for HIV/Aids, alcohol and drug dependency, depression, access to prenatal care, and lack of insurance. (New York Department of Health and Mental Hygiene, 2006) What became clear is that our research required a deeper look into the myriad of social, cultural, economic issues that underpin each of these public health issues. Looking at the urban ecosystem of health, we looked broadly across systems of policy, education, behavior, environmental factors, and issues of accessibility. While complex and interrelated, we began to identify factors that might support, mitigate, or inadvertently create barriers to health. While we found countless organizations that were supporting the community’s health, we also found countless system inefficiencies and mechanisms of ‘negative reinforcing loops’ that seem to lock individuals into a tireless cycle of hardship and poor health. Many of these negative loops can be attributed to industrial gain and ineffective policies and programs that are seemingly at odds with one another. It is no wonder that people choose to ‘opt-out’ of that system. In order to understand those system ‘disjunctures,’ we realized we would need to shift our thinking toward the individual needs of the community members.

Having started with the broad and messy, we narrowed our focus towards the Hunts Point community in areas with the strongest potentialities; and through this process, developed further research assemblages to explore further including: Education, Lifestyle/Behavior, Access, Support, and Funding. We were specifically interested in exploring potentialities that could exist at the community level while leveraging the ‘external mechanisms’ for community-based transformation. We went through several rounds of iterations, each time reframing our research questions around these assemblages in order to better understand the individual experience. Of utmost importance was the ability to allow for community-based projects to be implemented for and by members of the community.
In order to better understand the everyday challenges of the individuals in Hunts Point, we created a scenario building tool that would help us evaluate our research insights, and generate further ideas and questions. We developed personas for a mother, her two children, a teacher, and a bodega owner and then imagined their journeys throughout a particular timeframe within the context of the physical environment. Through the act of mapping a journey and their various interaction points within the community, the team can envision a possible future, and discuss interventions with a visual language. We also juxtaposed ‘five levels of influence’ on health related behaviors (taken from the public health model), as a means for assessing a specific idea. Each scenario can then be discussed and assessed through different means of impacting behavioral health.
1. intrapersonal factors: encompasses the knowledge, attitudes, and skills of the individual
2. interpersonal relations: includes family friends and coworkers and reflects peer pressures or support networks
3. institutional factors: where people spend one-third to one-half of their lives, such as school or work. In these settings, individuals may have profound effects on each others health and health-related behavior
4. community: organizations can work together in a community to jointly promote health goals
5. public policy: encompasses the regulations and limitations on behavior. These are the most explicit and controversial measures (Shneider)
{kind=link}
The scenario building framework, first and foremost, provides a means for generative discussion, while giving us a useful way to visualize them. We believe it will help our team to explore various interventions and ideas through common interests and variables. The variables of the scenario (time, place, or persona) can be interchanged and tested against different hypotheses, and then assessed through specific criteria such as the public health criteria listed above, or even another set of criteria. As we begin to prototype and test the tool further, we look forward to engaging community members into this conversation so that we can decipher what variables are most pertinent to explore. Through role playing and scenario planning, we are hoping to recontextualize our ideas towards actionable forms, whether they are sustainable action plans, initiatives, programs, or even simple health behavior choices at an individual level.
Sources
New York City Department of Health and Mental Hygiene, Community Health Profiles, Hunts Point and Motthaven, 2006
Birn, Anne-Emanuelle, Yogan Pillay, Timothy H. Holtz. Textbook of International Health: Global Health in a Dynamic World. New York: Oxford University Press, 2009
Meehan, Maggie , Yeh, Ming-Chin and Spark, Arlene, ‘Impact of Exposure to Local Food Sources and Food Preparation Skills on Nutritional Attitudes and Food Choices Among Urban Minority Youth’, Journal of Hunger & Environmental Nutrition, 3: 4, 456 — 471, 2008
Wilkinson, Richard. Unhealthy Societies: The Afflictions of Inequality. New York: Routledge, 1996.
Raphael, D. Social determinants of health: Present status, unanswered questions, and future directions. International Journal of Health Services 36(4): 651-677.
Schneider, Mary-Jane. Introduction to Public Health. Sudbury: APHA Press, 2011
Holloway, Kasey. Personal Interview. March 4. 2011.
Parkinson, Jay, MD. MPH. Personal Interview. March 3. 2011